







A lisp is often a red flag for a deeper problem. Find out how Orofacial Myology can help with proper diagnosis and treatment of this common articulation problem.
In the UK, lisps are not routinely treated by Speech Pathologists. In some places a lisp is regarded as a cosmetic problem and so may not be treated.
Many teachers aren’t identifying lisps in their students. Perhaps they think that it is normal in young children.
It is crucial that lisps are assessed and treated.
Yes, people with lisps may face problems with self-esteem and confidence. They may be discriminated against socially and in the workplace and be more readily overlooked in job interviews. They may be subjected to bullying because they sound different, and this may be either overt or subtle. Lisps matter to social, financial and emotional well-being of people.
But lisps have further implications for the health and well-being of a person. When the tongue is in the wrong place for a sound (eg. too far forward when saying s/z), we should be asking “WHY?”
WHAT IS A LISP?
There are different types of lisps. With an interdental lisp, the “s” sounds and looks like a “th”, with the tongue sticking through the teeth instead of contacting the bumpy alveolar ridge on the roof of the mouth behind the teeth. A dental lisp is a little harder to see, but the teeth touch the back of the teeth when saying s/z.
In traditional Speech Pathology practice, interdental and dental lisps are regarded as normal up until the age of about 4 ½.
However, a lisp can be a red flag for a more complex issue with the tongue.
A lateral “s/z” is where the tongue sides are flat rather than raised. It leads to a slushy sounding “s/z”. It is NOT a normal speech pattern at any age. This type of lisp may be associated with a submucosal (AKA posterior) tongue tie. A submucosal tongue tie may be difficult to detect and it is strongly recommended that a child with this sort of speech problem is assessed by a Speech Pathologist (or other professional) who is specifically trained in Orofacial Myology or assessing tongue ties.
TONGUE PROBLEMS ASSOCIATED WITH A LISP
The most common type of lisp (interdental or dental lisp) is associated with a low, forward tongue position. This is in contrast to the ideal position of the tongue, which is suctioned to the roof of the mouth, just behind the front teeth. I call this resting position the “sweet spot”, because getting the tongue to sit here at rest (ie. most of the time, with the exception of when we are talking or eating) is associated with so many health and development benefits.
What you may see when there is a low, forward tongue position is:
– Lisp (as described above)
– Other interdental sounds – the tongue may stick out through the teeth for a range of other sounds, such as n, l, t and d in addition to s and z. The only sounds in English that are made with the tongue sticking through the teeth (interdental) are voiced and unvoiced “th” (eg. in THose and THink). Therefore you should only see the tongue between the teeth when those sounds are being made.
– Open mouth posture with or without mouth breathing – the mouth may hang open rather than being closed at rest. The tongue may stick out between the teeth at other times, eg. when concentrating on something. This may look cute in littlies, especially when parents note that they take after their Mum or Dad, but it is actually a warning sign! (And yes, these tongue and airway problems often DO run in families!)
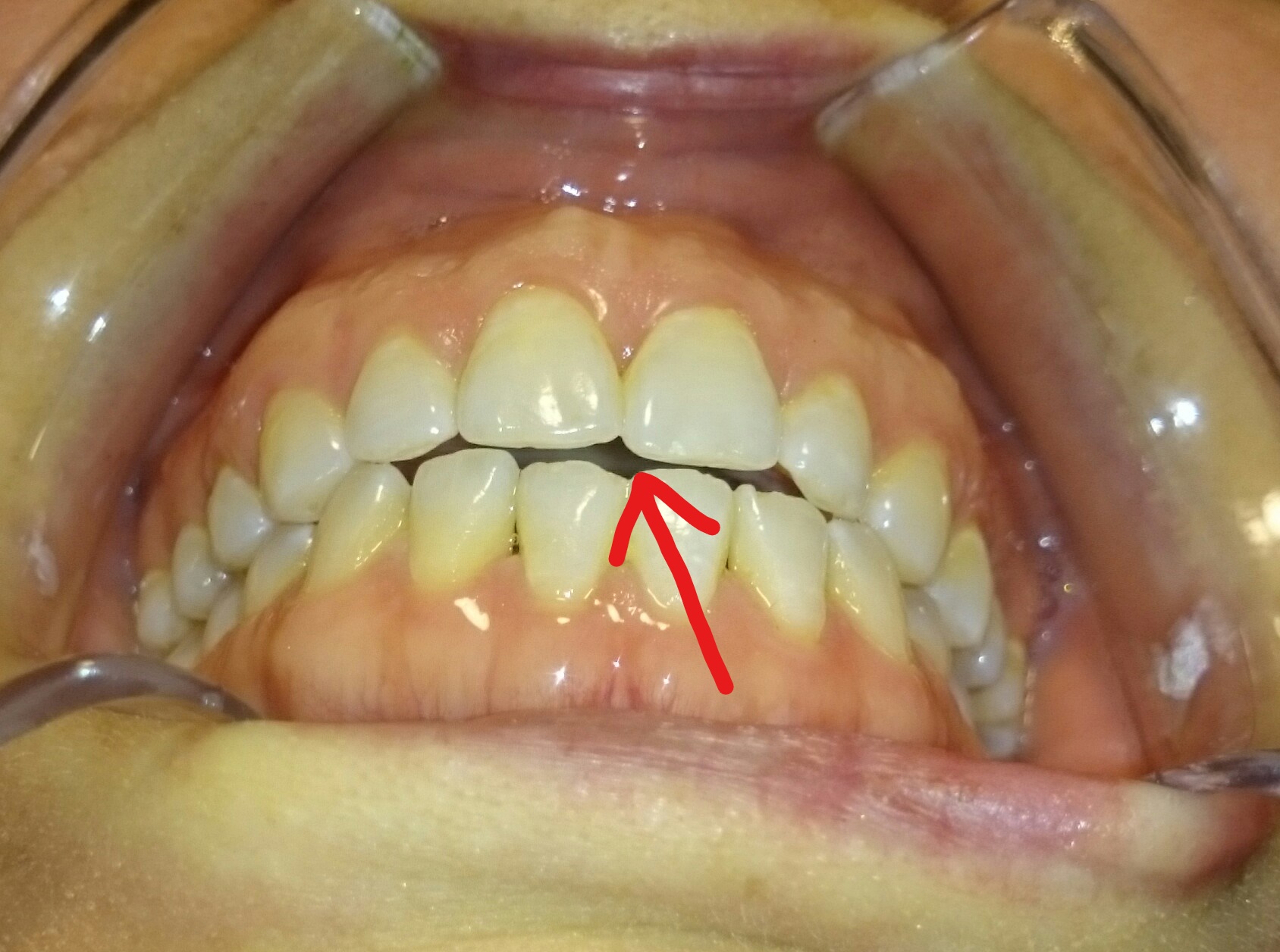
– Tongue thrust swallow – are you seeing your child’s food when they are eating? Can you see the tongue against the teeth or even through the teeth when chewing and swallowing? A tongue thrust swallow can be hard to spot, especially when the tongue is simply contacting the back of the teeth while the teeth are closed. Therefore you should get it assessed if you are in doubt. I worked as a Speech Pathologist for many years before detecting my own tongue thrust swallow. My tongue moves forward against my teeth when I swallow. I’m currently in the process of retraining this (though this requires multidisciplinary treatment, as there is a lot more than just the tongue thrust, since allergies, nasal obstruction, grinding, TMD and sleep disordered breathing are all also part of the picture). You can see the open bite that this constant force has caused on my teeth (the gap between top and bottom teeth in the photo below).
– Dental problems – open bite, molars resting lower than incisors, narrow dental arches leading to overcrowding of teeth and other malocclusions (problems with the closing of the teeth). Mouth breathing is associated with a high, vaulted hard palate and more problems which are outlined below.

MORE PROBLEMS!
Other potential complications of a low forward tongue resting position include poor posture (eg. forward-rounding of the shoulders), neck and back problems, restricted upper airways, sleep disordered breathing (including obstructive sleep apnoea) and snoring. Mouth breathing is associated with a range of health problems including breathing problems, disturbances to the pH balance in the gut, reflux, prolonged bed-wetting in children, bad breath, dental decay, enlarged tonsils and adenoid, TMD (temporomandibular joint disorder), chronic overbreathing, inefficient and tiring breathing patterns using upper chest, crowded and crooked teeth, and low tone in lips which may lead to swallowing problems.
It may take many years for this cascade of negative events to occur.
The tongue can exert a force of approximately 500g on teeth, whereas 10-15g is regarded as a significant force that is capable of moving the front teeth. It’s not surprising then that the tongue position and its repetitive, frequent patterns of movement can have such a significant influence on the development of the jaw and teeth.
WHAT CAUSES PROBLEMS WITH TONGUE POSITION AND TONGUE THRUST
There are many reasons why a child (or adult) may have their tongue in a low, forward tongue position. This includes tongue tie and restricted airway due to enlarged tonsils and/or adenoid, turbinates and deviated septum. Allergies should be assessed, particularly in people showing signs of allergies such as lines under the eyes (Dennie Morgan lines) and dark rings under the eyes (venous pooling). People with a restricted upper airway may move the tongue forward habitually in order to enlarge the airway behind the tongue.


A low forward tongue position can persist even after obstructions (eg. enlarge adenoid) are cleared. In a group of children with tongue ties and sleep disordered breathing, many of the children’s complaints (the chief one being fatigue) persisted after surgery or orthodontic work. However, 4-6 months of myofunctional therapy led to resolution of problems for all of the children (Huang et al, 2015). It is essential that the tongue position and patterns of movement are corrected, as well as nasal breathing restored – and orofacial myology (AKA myofunctional therapy) can help with this.
Sucking and biting habits can also be part of the picture. In particular, sucking a thumb or dummy reinforces a low, forward tongue position. Sometimes sucking habits can be a compensation for airway problems, as they help to enlarge the space behind the tongue (pharynx) to facilitate breathing.
WHY LISPERS SHOULD BE ASSESSED BY AN OROFACIAL MYOLOGIST
Orofacial myologists are well-placed to assess and treat problems with the tongue, such as tongue thrust and habitual low, forward tongue resting position. Finding an orofacial myologist who is also a Speech Pathologist is a bonus, because of their additional understanding of articulation.
One of the goals of myofunctional therapy is to correct dysfunctional tongue habits. This is crucial. A person swallows up to 3000 times per day. If someone is reinforcing a forward tongue position through a tongue thrust swallow that many times per day, then correcting a lisp through articulation work is going to be an uphill battle, that many people will lose.
And, it is missing the point. In people with airway and/or tongue problems, the lisp is the SYMPTOM, not the real problem. Let’s start looking at the real cause, and stop offering a bandaid solution.
FOR MORE INFO:
Orofacial Myofunctional Disorders – American Speech, Language and Hearing Association (ASHA)
Orofacial Myology blog – for Speech Pathologists and Orofacial Myologists



{kind=link}
Susie, this article brings a tear to my eye as it describes my son. My lovely speech therapist has described this too me but says there are so few speech therapists trained in Orofacial Myology. Do you know of anyone in Melbourne that may be able to help him?
Thank you for such an explanatory article!
Hi Tracy! Sorry for the delay in my reply and thank you for sharing your experience. There are some great therapists in Melbourne who are trained in both Speech Pathology and Orofacial Myology. I’ll email you details. All the best!
hey im 15 and i have the s/z lisps and i tried some tips but they never seemed to really work , i tried to raise the sides of my tongue so they touch my upper teeth on the sides of my mouth but didnt work the s was not clear and it was too much effort and i think all of this is because i have a gap between my upper teeth , what can i do to get rid of my lisp ??
p.s : some people told me i sould do braces and my dentist said i shouldnt do so but he never noticed i have a lisp .
thank you
Hi! Good on you for reaching out. I suggest you see a Speech Pathologist (also known as Speech Language Pathologist or Speech Therapist) for an assessment. In my professional opinion, a Speech Pathologist who is trained in and experienced with Orofacial Myology will be best suited to help you, as a lisp indicates a tongue problem, and you also mention possible dental/orthodontic issues. I could give you tips to improve the issue, but sometimes there are underlying or accompanying issues to address first, to give the best chance of improvement. You can find Orofacial Myologists on iaom.com. Not all Orofacial Myologists are Speech Pathologists, but since the lips is your main concern, it would be best to find an OM who is a Speech Pathologist. Many OMs are not registered with the IAOM, so if you can’t find someone near to you, shoot me an email and I’ll see if I can find someone for you. All the best! Susie